© Jonathan Ross / Getty Images

© "Kennebunkport, ME" by pvsbond is licensed under BY-SA 2.0.

© Joseph Sohm/Shutterstock.com

© "Steamboat Springs, CO" by acertainworld is licensed under BY-SA 2.0.

© "Feb 1, 2009 - Big Sky, Montana" by Dennis from Atlanta is licensed under BY-SA 2.0.

© "Colorado - Dillon - August 1972" by Ladycliff is licensed under BY 2.0.

© U. Eisenlohr/Shutterstock.com
© Matt Gush/Shutterstock.com

© Magargee Films/Shutterstock.com

© SR Productions/Shutterstock.com

© "Moonstone Beach, Cambria CA" by Mr Phil Price is licensed under BY-SA 2.0.

© iStock.com/Jonathan Ross

© Kevin Ruck/Shutterstock.com

© "Roche harbor, San juan islands WA" by M I K E M O R R I S is licensed under BY-SA 2.0.

© "Petersen Village Inn, Solvang, CA, USA (9500336893)" by l0da_ralta is licensed under BY 2.0.

© "Groton Long Point CT" by Rusty Clark ~ 100K Photos is licensed under BY 2.0.

© "Bay Avenue, Green Harbor MA" by John Phelan is licensed under BY 3.0.

© "Near Minturn, CO (2)" by Cyndi and Dave is licensed under BY 2.0.

© Alexander Lukatskiy/Shutterstock.com

© topseller/Shutterstock.com

© "Sailboats on the beach at Sunrise - Sea Isle City, NJ" by holl7510 is licensed under BY 2.0.

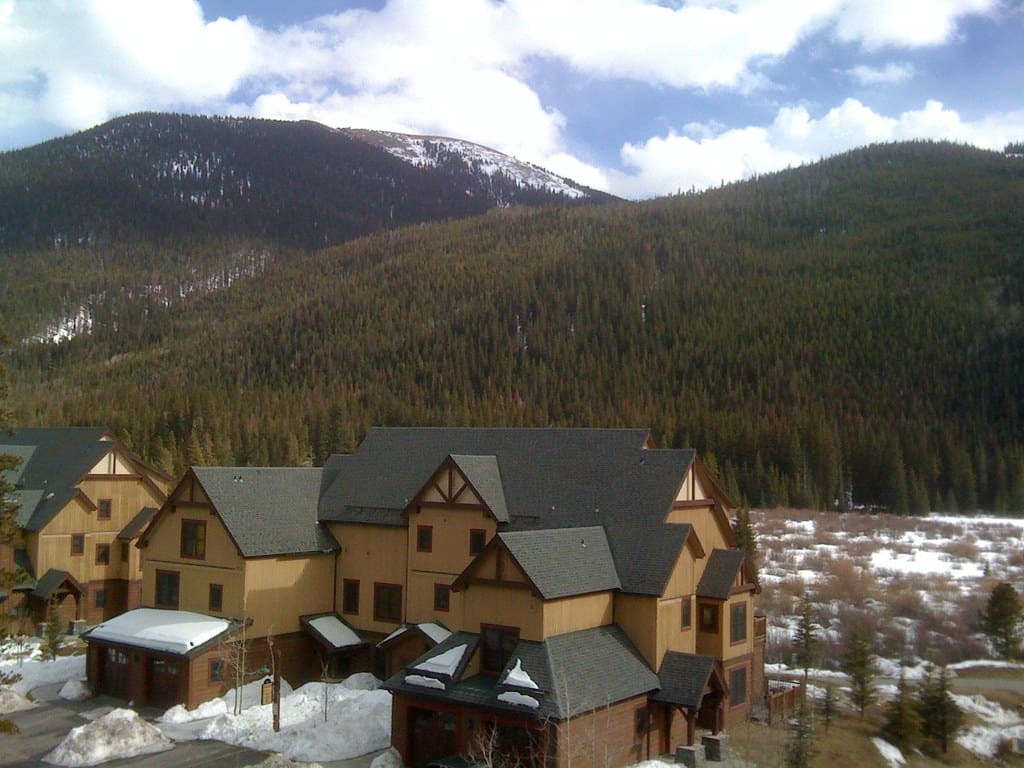
© "Breckenridge, CO" by Jasen Miller is licensed under BY 2.0.

© "Splash! Estero Bluffs SP, just north of Cayucos, CA. Bonus: Cayucos Deli!" by Pete Tillman is licensed under BY-SA 2.0.
© Ingo70/Shutterstock.com
© "Keystone, co" by sebrenner is licensed under BY 2.0.

© "Teton Pass, Wyoming Highway 22, Near Jackson, Wyoming" by Ken Lund is licensed under BY-SA 2.0.

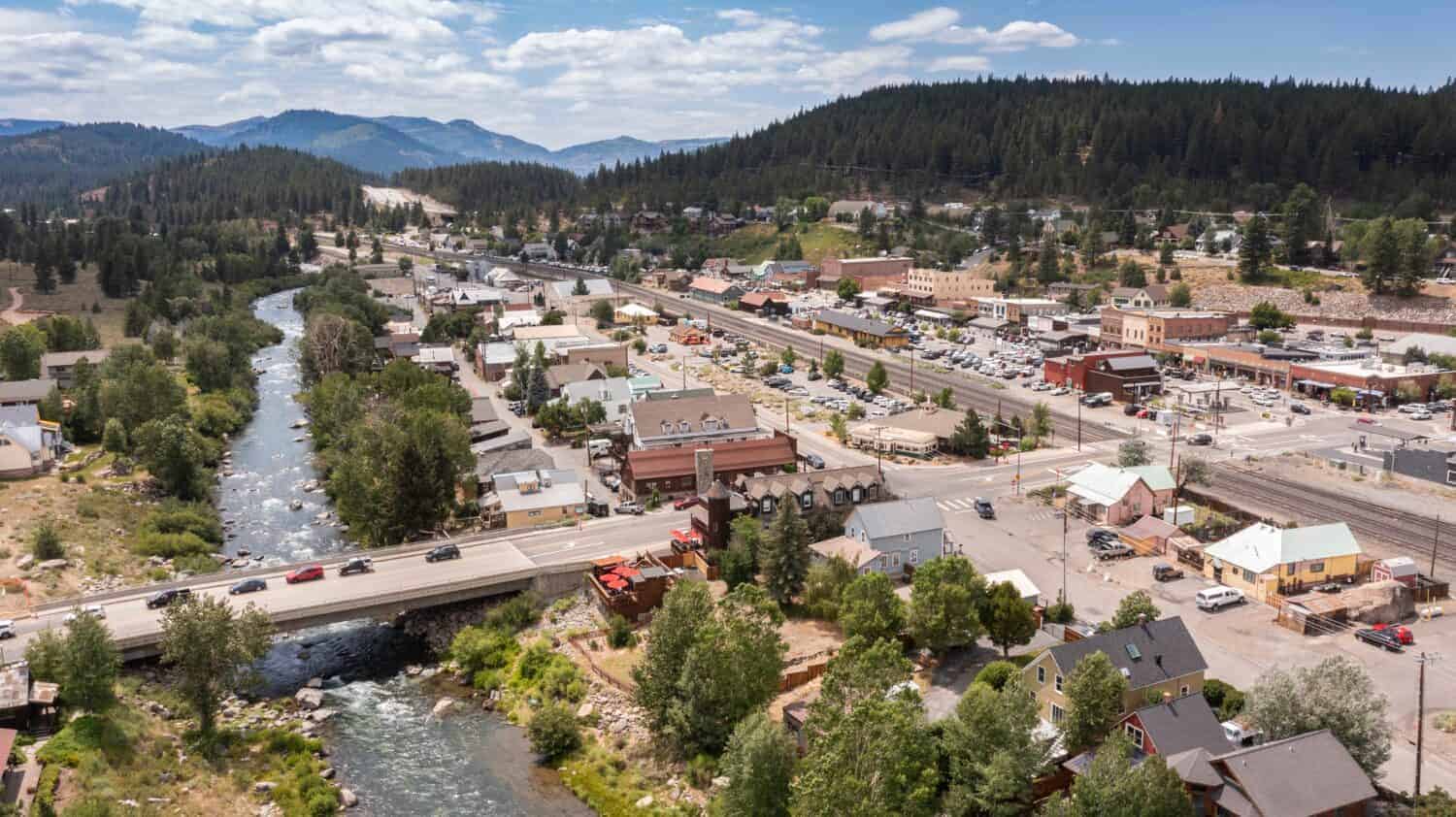
© "Truckee River Near Tahoe City, California" by Ken Lund is licensed under BY-SA 2.0.

© CSNafzger/Shutterstock.com

© "Lake Tahoe, California, United States" by Giuseppe Milo (www.pixael.com) is licensed under BY 2.0.

© Kirk Fisher/iStock via Getty Images

© "Welcome to New Jersey" by bobbsled is licensed under BY-SA 2.0.

© iStock.com/stockphoto52

© "Hills in Tres Pinos, CA" by DoNotLick is licensed under BY 2.0.

© "Little Duck Key FL 7 Mile Bridge02" by Ebyabe is licensed under BY-SA 3.0.

© "Bridlewood Estate Winery - Santa Ynez, CA" by Christian Mesiano is licensed under BY-SA 2.0.

© "Welcome to South Carolina" by paulhami is licensed under BY-SA 2.0.

© bodrumsurf/Shutterstock.com

© CanyonOaksMedia/Shutterstock.com

© "Kawuneeche Valley, Rocky Mountain National Park, Colorado" by Ken Lund is licensed under BY-SA 2.0.

© "US 89 WY Hoback Jct" by Rschen7754 is licensed under BY-SA 4.0.

© "(Another) Trail Creek Campground, Alta, WY" by dvs is licensed under BY 2.0.

© TeBe Inspires/Shutterstock.com

© "Tabernash, CO-funny house" by Cyndi and Dave is licensed under BY 2.0.

© "Sunset in Avila Beach, CA. Picture taken from our hotel." by Marc van der Chijs is licensed under BY-ND 2.0.

© Alexander Lukatskiy/Shutterstock.com

© "Snow in Los Olivos, CA (MVC-116S)" by Willscrlt is licensed under BY-SA 2.0.
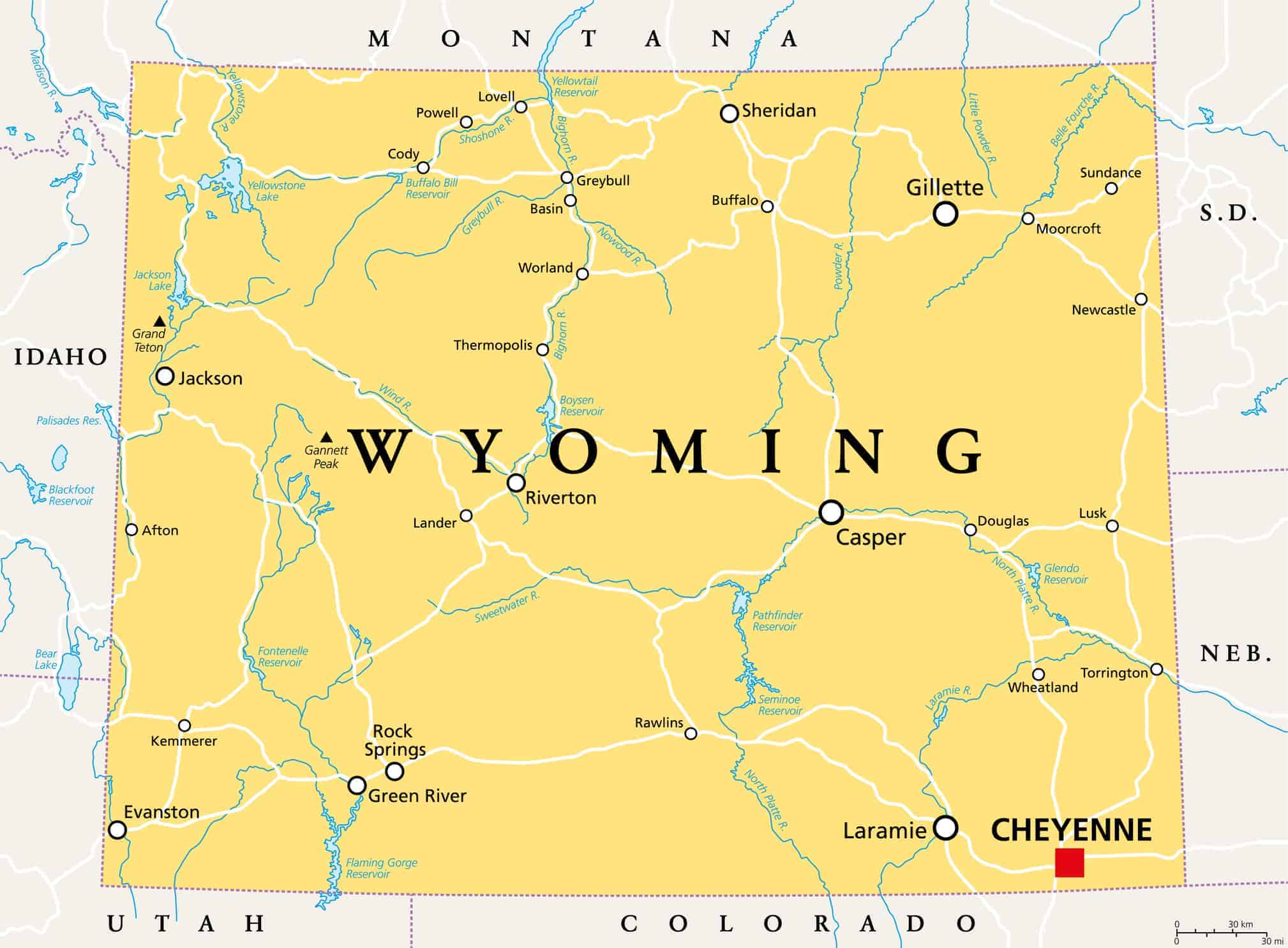
© PeterHermesFurian/iStock via Getty Images

© "Wave crashes on the rocky shore at Shell Beach north of Bodega Bay, CA" by northbaywanderer is licensed under BY-SA 2.0.

© "START Bus in Teton Village" by Crystalmountainskier is licensed under BY-SA 3.0.
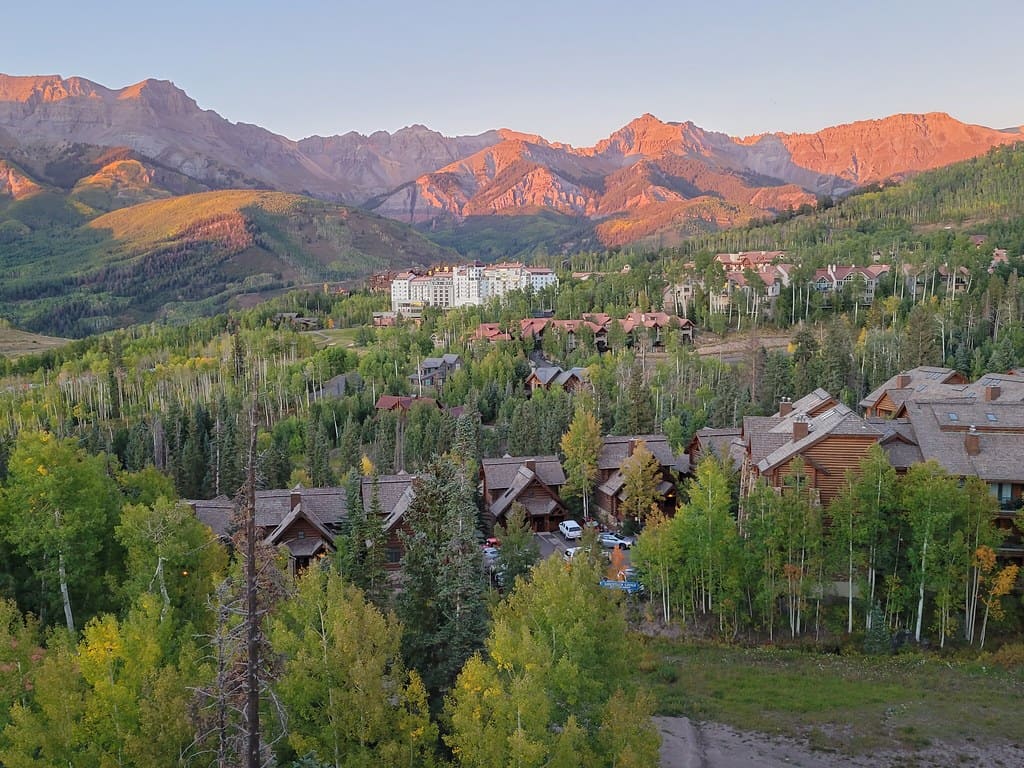
© "Dusk at Mountain Village, CO" by Moo.The.Cow is licensed under BY 2.0.

© "Grizzly on Moose-Wilson Road" by GrandTetonNPS is licensed under PDM 1.0.